
Last November, I was working in collaboration with a consultant from Johns Hopkins University to build a costing model for our Mobile Technology for Community Health (MOTECH) program. MOTECH has 2 major components:
- A voice and SMS service that sends time-based messages to pregnant women and new mothers about maternal and newborn health and reminds them to seek appropriate healthcare
- A Client Data Application that is used by Ghana Health Service healthcare practitioners to track patient data, be alerted of missed patient appointments, and streamline their monthly reporting process (normally a tedious, manual process in paper registries)
Together, we visited the Gomoa West district to interview some Ghana Health Service staff who had been a part of MOTECH and find out what went into piloting MOTECH in their district, including the costs associated.

Lisa (right) and Michelle (John Hopkins consultant) meeting witha Ghana Health Service staff.
After meeting with the administrative staff, we asked to see a Community-based Health Planning and Services (CHPS) facility in a nearby village to learn firsthand how patient management was conducted and see what resources the community health nurses had. Ghana Health Service introduced the CHPS initiative in the early 2000s to decentralize healthcare provision to the community level since geographic access is a major barrier to healthcare and contributes to high childhood mortality. As much as I had researched and analyzed Ghana’s healthcare system from a desk, I had never stepped foot in a CHPS compound before, and wasn’t sure what to expect. We drove on bumpy dirt roads into the rural area for about 20 minutes and came upon a small CHPS clinic that serves the surrounding community in Gomoa Kumasi/Obokrom. While two nurses were staffed there, only one of them, Esther, was available to meet us that day.

Joseph (MOTECH staff), Lisa, and Esther (nurse) at teh CHPS facility in a rural community.
It was unlike any clinic I’d ever seen. Three rooms comprised Esther’s entire facility: her modest living quarters, a patient intake room outfitted with counseling materials, scattered plastic chairs, and a wooden medicine cabinet and finally, the emergency delivery room – where women who couldn’t make it to a district hospital delivered their babies. All with no running water and spotty electricity, leaving the compound blanketed in a heavy, uncomfortable heat.

Esther (nurse) in her patient intake room with at Mobile Midwife poster on the wall.
As I stepped into the delivery room, I was shocked at how barebones it was compared to the ones I was accustomed to in North America with fancy equipment and sterile instruments. On the right hand side was a wooden table, covered with a plastic tarp sheet, where the pregnant woman would lie during childbirth. Separated by a makeshift divider on the left was another table with a keg of water on top, a plastic basin, a couple of chairs, and some drawers of medical instruments like forceps and scissors. I couldn’t believe that was it! I asked Esther how many women had given birth in this delivery room that month and the answer was three. They were considered lucky to have made it into the clinic, rather than delivering unassisted at home, where most complications and maternal deaths tend to occur.

Emergency delivery room in the CHPS clinic with the delivery table on the right.
Afterwards, we chatted with Esther about what it’s like working in the community, which she shared could get lonely at times since she’s far away from her family and friends and doesn’t get to see them often. As a frontline health worker, she handles any and all cases that arise in the community, from malaria to infant diarrhea to youth sexual/reproductive health counseling, while the more complex cases are referred to larger district hospitals. I thought about how well she fit the user persona for our “Community Health Nurse – On the Go” app, which is still piloting in select districts but could scale nationwide.
As we were leaving, I noticed a hand-drawn pinwheel and map taped outside the clinic. Esther explained that she had drawn a neighborhood map to facilitate home visits for patients who called in and the pinwheel was to inform walk-in patients about the nurses’ whereabouts. Who says technology has to be the solution to everything? Quite creative on her part!
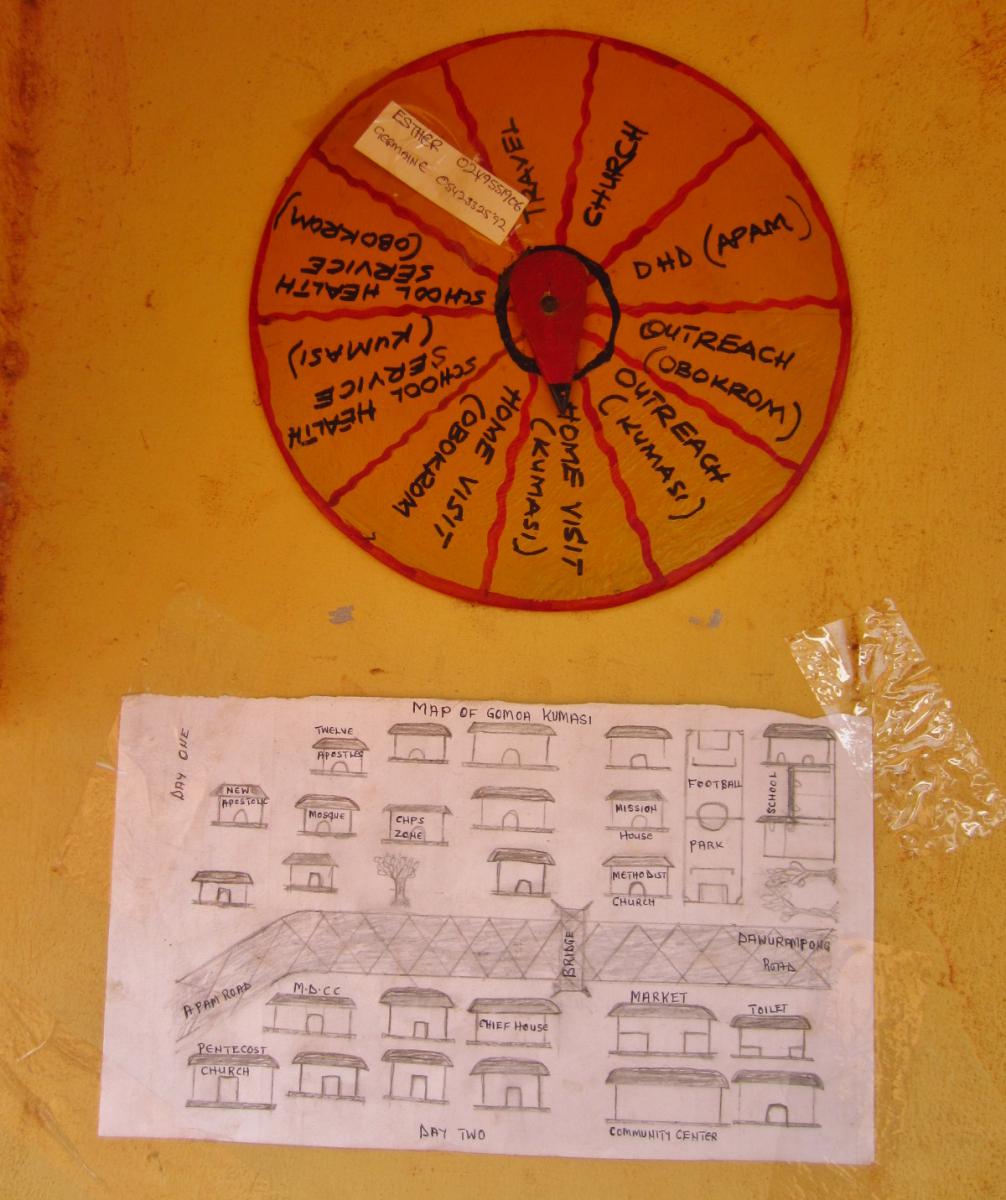
Esther's "out of clinic" pinwheel and hand-drawn map of her community.
Suffice to say, visiting the Gomoa West district and meeting a frontline healthcare worker was a humbling experience I’ll never forget. As rough as life gets in Accra with the stifling heat and 24-hour power outages, I can’t imagine having to take care of patients in those conditions as well. I can only hope mobile health initiatives like Grameen Foundation’s can make her daily work a little bit easier.
Tune in next time as I write about my Takoradi field trip to recruit new users with the No Yawa team!
Lisa Wei is Grameen Foundation’s Mobile Health Strategy Fellow. She is based in Accra, Ghana and can be reached at lwei@grameenfoundation.org.